My health journey: Jane MacDonald
Jane MacDonald: My Type 1 Diabetes Lived Experience

I’m happy to share my 27 years of lived experience with Type 1 Diabetes, having been diagnosed at age 35 during my first pregnancy.
The current standard of practice for people with Type 1 Diabetes involves a high-carbohydrate and large-insulin-dosing protocol that results in outcomes of high and unpredictable blood glucose and, therefore, diabetic complications.
I have enjoyed blood glucose levels in the non-diabetic range for the past 8 years, using half the insulin I previously required. I have managed to reverse inflammation and the diabetes-related health conditions and cognitive burdens I was formerly experiencing. I have achieved this by avoiding what my body cannot metabolise, chains of glucose molecules, or carbohydrates. I practice Therapeutic Carbohydrate Reduction (TCR). I do this by eating real, whole foods; avoiding ultra-processed foods; and reducing carbohydrate and sugar intake.
This approach helps me avoid the two biggest risks of diabetes emergencies: diabetic ketoacidosis and severe hypoglycaemia, as well as steering clear of living with the ‘ticking time bomb’ of diabetes, which is the leading risk factor for many other health conditions.
This way of life is achievable and sustainable, as my continuous 8-year achievement demonstrates. When I initiated this lifestyle, I lost the 14 kilograms that insulin use over 20 years had caused. This was a bonus.
I am frustrated that the standard of care for type 1 diabetics follows the 2013 Australian Dietary Guidelines. The Australian Dietary Guidelines’ objectives are to promote health and wellbeing, reduce the risk of diet-related conditions, and reduce the risk of chronic disease. The statistics highlighting the alarming rise in obesity and Type 2 Diabetes, the increased demands for diabetes and obesity medications, costing the Commonwealth billions of dollars, make it clear that these objectives are not being met.
Following the current so-called ‘’healthy” food pyramid has led to Australians becoming more insulin resistant, leading to poorer health outcomes for many. To quote one medico: “You live by the pyramid, you die by the pyramid and along the way you end up looking like the pyramid.”
I note that page 2 of these Dietary Guidelines clearly states: “These Guidelines do not apply to people with medical conditions requiring specialised dietary advice”. Yet diabetics, who can’t metabolise carbohydrates, are advised to follow these guidelines, making carbohydrates the basis of every meal. This is setting diabetics up to fail, and to a lifetime of roller-coaster blood sugars and diabetes-related complications, to anxiety, depression, and to a lesser quality of life.
TCR as a management tool for Type 1 Diabetes is not new. The ‘Law of Small Numbers’ method is extensively outlined in Dr Richard Bernstein’s book ‘The Diabetes Solution’, originally published in 1997, 29 years ago! This method significantly decreases the margin of error when using insulin. It increases time-in-range for blood sugar and reduces standard deviation by significantly reducing variation in blood glucose levels. It leads to flat, smooth lines on my Continuous Glucose Monitor (CGM). No more roller-coaster blood sugars! The first two photos below show a typical day pre-TCR, and the photo on the right demonstrates how my blood sugar generally looks now. I no longer experience hypoglycaemia, seemingly coming from nowhere. On three occasions, I had hypoglycaemic events which would have been lethal had I been alone. I don’t have to fear this anymore.

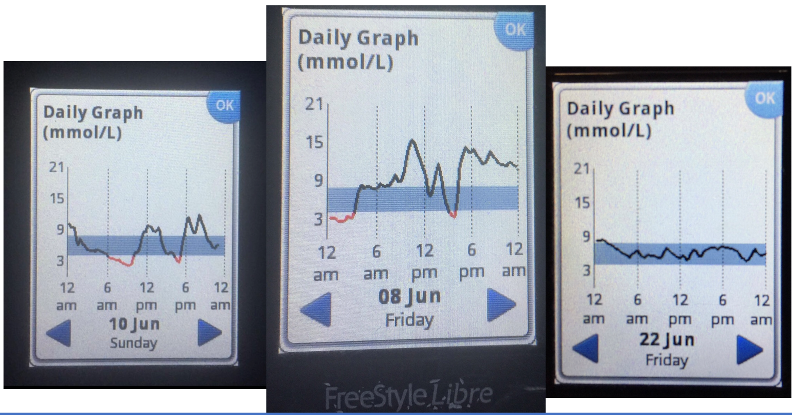
Additionally, Dr Bernstein clearly explains how diabetics can dose insulin for eating protein, fat, and carbohydrate. Sadly, I was living with T1Diabetes for 20 years before I happened across this method, via YouTube and Facebook.
I had never been educated as a patient about the benefits of TCR, the natural interplay between glycogen and glucagon in response to eating protein, and how this can cause blood glucose levels to rise 2-6 hours after ingesting protein, requiring an adjustment in insulin dosing. I had never been educated about the impact fat has on insulin sensitivity.
I dreaded my regular medical appointments, including visits with my Endocrinologist and Diabetes Educator. I felt like a failure. Even though I had diligently followed all the medical, pharmacological, and dietary advice I was given, my results remained significantly suboptimal.
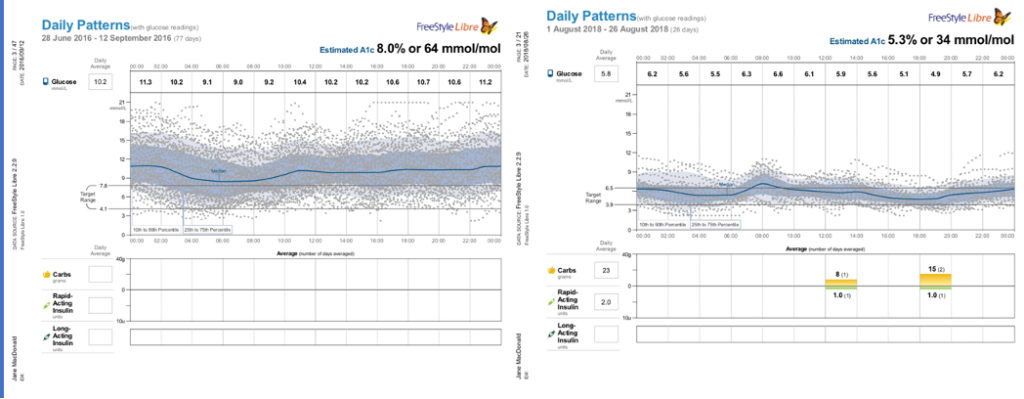
The benefits of TCR and Dr Bernstein’s insulin protocols on my blood sugar were almost immediately obvious on my continuous glucose monitor. The photos below show my CGM readings before and after adopting these changes
This makes me question whether the current diabetes Standard of Care involves the basic tenets of medicine. The tenets of patient-centred care, informed consent, best-practice guidelines, and evidence-based medicine. How could these apply when much of what I now know was never communicated to me during 20 years of medical appointments and is still not reflected in current patient education on diagnosis? Current statistics around the rise in diabetes and obesity suggest that even the first tenet of medicine, “Do no harm”, is failing.
I am not a medico, but fortunately, my health literacy was adequate to work out how to adjust my insulin regimen to achieve the results I have benefited from. I did this when I was not adequately supported by my previous Endocrinologist as I transitioned to TCR and Dr Bernstein’s insulin dosing regimen. I firmly believe that this knowledge should be offered to all diabetics as part of the Standard of Practice.
It is encouraging that TCRis finally being recognised as an appropriate management tool for Type 2 Diabetics. Change has been slow, but thankfully, it is starting to happen. Examples of this are:
- In Nov 2021: Remission of Type 2 Diabetes was acknowledged in Australia’s ‘National Diabetes Strategy’ for the first time.
- In Sept 2023: Australia’s first public hospital Remission Clinic for People Living with Type 2 Diabetes opened at the Royal Melbourne Hospital, and
- In Dec 2023: Guidelines for the Remission of Type 2 Diabetes were endorsed by Diabetes Australia, with their publication entitled- Managing Type 2 Diabetes with Therapeutic Carbohydrate Reduction.
However, although TCR is increasingly included as an option, it often comes with caveats and cautions that discourage clinicians from recommending it, and the emphasis on carbohydrates remains the norm. One example of this is the carbohydrate recommendations in the Nutrition Guide for Children with Type 1 Diabetes, published by Queensland Health, which recommend that children aged 14 years and older eat up to 300 grams of carbohydrates per day. This is equivalent to 75 teaspoons of sugar!
I am grateful to have found a very supportive Type 1 Diabetes online community that educated me when I wasn’t supported by my medical team at the time. The Facebook groups Typeonegrit, with almost 4,000 members, and Typeonenormal, with almost 5,000 members, allow international communication with fellow Type 1 Diabetics and their carers who use this management tool.
I am grateful to have since found a very supportive Endocrinologist and Diabetes Educator, both of whom support the TCR approach as a Type 1 Diabetes management tool. Australia is lucky to have a large cohort of Doctors and Allied Health Professionals who understand the TCR approach for Type 2 and Type 1 Diabetics, and they are educating their patients accordingly. I believe the Australasian Metabolic Health Society doctors would be well placed to form a Taskforce to steer the way forward for all Australian diabetics.
I submitted to the 2024 Parliamentary Inquiry into Diabetes in Australia. I was thrilled to be invited to appear before the Committee at Parliament House, chaired by Paediatrician and Parliamentarian, Dr Mike Freelander. I thanked the Committee in advance for its recommendations to improve the lives of Australians living with diabetes. I asked them to please ensure three things:
- A change to dietary recommendations for diabetics, so that all diabetics are advised according to what will provide them with optimal health outcomes- a far cry from the current situation.
- The implementation of a low-carbohydrate protocol, allowing Type 1 Diabetics to live long-term with normal blood sugars, meaning that people living with Type 1 Diabetes are ensured access to quality information, choice and support.
- The revision of current education of doctors and health practitioners providing support for diabetics, avoiding conflicts of interest with pharmaceutical and ultra-processed food companies, to improve patient-centred care, informed consent, best-practice guidelines, and current evidence-based medicine.
According to Diabetes Australia, approximately 134,000 Australians (0.5%) live with Type 1 Diabetes, and diagnosis rates are rising. These changes could significantly improve the physical and mental health of so many, as well as their quality of life, and would save billions of dollars from Health budgets. There would be significant personal, community, and Commonwealth fiscal benefits, allowing for better health for generations of Australians.
I was disappointed that the “The State of Diabetes Mellitus in Australia in 2024, House of Representatives Standing Committee on Health, Aged Care and Sport” Parliamentary Inquiry Final Report didn’t include TCR as a recommended option for Type 1 Diabetics. It did, however, mention my use of TCR. It also included one of my quotes about diabetes burnout: “Type 1 diabetes is managed through blood glucose monitoring and insulin replacement. Ms Jane MacDonald, who has lived with Type 1 diabetes for more than 20 years, described the experience of managing Type 1 diabetes as ‘…an unrelenting cognitive burden… with us 24/7, 365 days a year. There is no holiday from diabetes, no break, and it can be challenging and exhausting.’”
Whilst TCR is now accepted as a legitimate and effective management method for Type 2 Diabetics, I believe my 8 years of safe and sustainable results demonstrate that this is a valid technique to also manage Type 1 Diabetes. I believe that Type 1 Diabetics deserve the tools that allow them to live with normal blood sugar, leading to an improved quality of life and no diabetes complications or diabetes burnout.